You will be given a comprehensive eye examination, including some tests especially tailored to evaluate whether your eyes are appropriate for the corrective surgery. From the results of this exam, the doctor can work with you to decide if LASIK is the right choice for you.
It is important to realize that, like any surgery, LASIK is not without risk. However, major complications are extremely rare. Minor complications occasionally occur, such as dry eye, and halos or glare around lights at night. However, such problems are uncommon, are often treatable, and will usually reduce or disappear within months of the surgery.
There is no pain associated with the LASIK procedure. Local anesthesia is used on the cornea, which is administered through eye drops. Some patients may experience mild discomfort or pressure. After the procedure, patients may experience minor irritation in the eye. This should fade within a day or two.

If you are considering LASIK eye surgery, it means you are living with nearsightedness, farsightedness or astigmatism, and probably currently wear glasses or contact lenses. LASIK is a great way to reduce your dependence on, or completely free yourself from, corrective lenses. It may be especially appealing because of your profession or lifestyle. It could be that you cannot wear contact lenses and dislike the appearance of glasses, or you may just want to reduce the expense and hassle of glasses and contacts. However, LASIK is not appropriate for everyone. There are several factors which determine the best candidate, including age, medical history, individual eye anatomy, and expectations. Each person is a unique case requiring individual evaluation.
No website can tell you for sure if you are a good candidate for LASIK. The only way to find out is to schedule a LASIK eligibility exam.
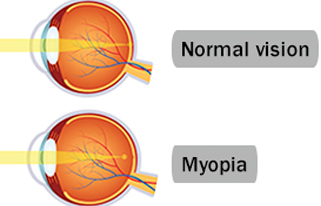
Myopia (short-sightedness) is a vision defect resulting from the eye being too long from front to back, or from the cornea (the clear part of the front of the eye which allows light in) being too steeply curved.
Myopia causes distant objects to appear blurred, whilst close objects can still be seen clearly.
Myopia usually appears around puberty, but may appear at any age from early childhood up to the age of 25. In most cases, myopia will stop getting worse when the growth process has been completed.
The earlier myopia starts, more severe it is likely to become. Myopia that starts in early childhood often gets worse in adult life, and may become very severe. Known as high degree myopia (or sometimes as pathological myopia), it can create problems in later life because of its association with changes at the back of the eye (Retina).
There is a tendency for myopia to run in families. Children have about a 30% chance of developing myopia if one of their parents has the condition, and a 55% chance if both have it. High degree myopia also runs in families.
Myopia can usually be corrected with glasses (spectacles) or contact lenses. These cancel out the increased curvature of your cornea or the increased length of your eye so that distant objects no longer appear blurred.
Surgery to correct myopia is available. It works by altering the shape of the cornea so that the eye focuses correctly.
If you have high degree myopia you are more likely to develop eye Disorderss in later life, such as retinal detachment, glaucoma, and cataracts.
A detailed eye examination (preferably by a retinal specialist) should be done every year.
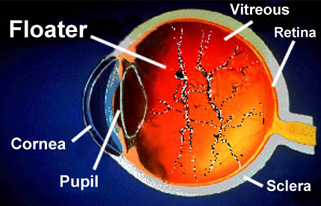
Occasionally, you may see small spots in your field of vision. These are commonly known as floaters. Floaters appear in various forms, such as dots, threads or cobwebs. Since they are within the eye, floaters move as the eyes move; they may dart away when you try to look at them.
A clear gel(vitreous gel) called the vitreous body fills the inside of the eye. If some of this gel forms clumps, floaters can result. Small flecks of protein or other material that were trapped in the vitreous during the eye's formation can also cause floaters. Even though they may seem to be in front of the eye, floaters actually are seen as shadows by your retina. The retina is the light-sensitive, inner layer of the eye.
Over time, the vitreous gel shrinks and may detach from the retina. The pulling can cause tiny amounts of bleeding. This is a common cause of floaters in people who are very nearsighted or who have had a cataract operation. Less often, floaters may result from other eye surgery, eye disease, eye injury or crystal-like deposits that form in the vitreous.
Seeing flashes of light is usually not cause for alarm. However, this may indicate a medical condition that can threaten your sight. It is best to take these and any changes in your vision seriously until a doctor tells you otherwise.
- Flashes of light that are accompanied by new floaters or a partial loss of the field of vision may be a medical emergency. Have your eyes examined immediately by an eye doctor to see if you have a retinal tear or detachment.
- Light flashes can also occur when the vitreous inside the eye shrinks and pulls on the retina. Flashes of light or jagged lines usually appear on and off for several weeks after the vitreous/retinal separation.
- Flashes of light may also be caused by migraines. If flashes of light are present in one or both eyes and last between 10 and 20 minutes, it may indicate a migraine, which is caused by a spasm of the blood vessels in the brain. This may be followed by a migraine headache. It is possible to have flashes of light or blind spots without the headache (sometimes called a classic or ophthalmic migraine)
Most people sometimes see spots, and these can become more noticeable with age. Surgical removal of floaters is rare and suggested in only the most severe cases. Often, people simply learn to ignore their floaters. If a floater appears in your line of vision, move your eyes around. This causes the fluid inside the eyes to shift and allows the floater to move out of the way. Since we usually move our eyes from side to side, looking up and down may be more helpful in removing floaters from your line of sight.
If you have a few floaters, it generally means that you may not have a serious eye problem. However, if a large number suddenly appear, or they seem to worsen over time, it is crucial to get an eye examination. If the floaters appear together with flashes of light or if you experience any vision loss, it might be a sign of serious conditions, which could threaten sight and would require immediate medical attention!
A complete eye examination will help determine the seriousness of floaters and the health of your inner eye. During a complete eye exam, called a dilated eye exam, the eye doctor widens the pupil of the eye with eye drops to allow a closer look at the inside of the eye.
Age-related macular degeneration (AMD) is a deterioration or breakdown of the eye’s macula. The macula is a small area in the retina — the light-sensitive tissue lining the back of the eye. The macula is the part of the retina that is responsible for your central vision, allowing you to see fine details clearly.
Even though the macula makes up only a small part of the retina, it is much more sensitive to detail than the rest of the retina, called the peripheral retina. The macula is what allows you to thread a needle, read small print, and read street signs. The peripheral retina gives you side (or peripheral) vision.
If someone is standing off to one side of your vision, your peripheral retina helps you know that person is there by allowing you to see their general shape. It is your macula that allows you to recognize the details of the person’s face.
Many older people develop macular degeneration as part of the body’s natural aging process. There are different kinds of macular problems, but the most common is age-related macular degeneration.
The retina is made up of many layers that work together to help you see clearly. AMD develops when a layer under the retina called the retinal pigment epithelium (RPE) is affected by deposits of tiny yellow or white pieces of fatty protein called drusen, or by other age-related changes.
With AMD, you may have blurriness, dark areas or distortion in your central vision, and perhaps permanent loss of your central vision. It usually does not affect your side, or peripheral vision. For example, with advanced AMD, you could see the outline of a clock, yet may not be able to see the hands of the clock to tell what time it is.
AMD alone almost never causes total blindness. People with more advanced cases of AMD continue to have useful vision using their side, or peripheral vision. In many cases, macular degeneration’s impact on your vision can be minimal.
When AMD does lead to loss of vision, it usually begins in just one eye, though it may affect the other eye later.
Many people are not aware that they have macular degeneration until they have a noticeable vision problem or until it is detected during an eye examination.
AMD alone almost never causes total blindness. People with more advanced cases of AMD continue to have useful vision using their side, or peripheral vision. In many cases, macular degeneration’s impact on your vision can be minimal.
When AMD does lead to loss of vision, it usually begins in just one eye, though it may affect the other eye later.
Many people are not aware that they have macular degeneration until they have a noticeable vision problem or until it is detected during an eye examination.
Dry, or atrophic, AMD (also called non-neovascular AMD)
Most people who have AMD have the dry form. This condition is caused by aging and thinning of the tissues of the macula. Macular degeneration usually begins when tiny yellow or white pieces of fatty protein form under the retina. These deposits are called drusen. Eventually, the macula may become thinner and stop working properly. With dry AMD, vision loss is usually gradual.
People who develop dry AMD must carefully and constantly monitor their central vision. If you notice any changes in your vision, you should tell your ophthalmologist right away, as the dry form can change into the more damaging form of AMD called wet (exudative) AMD.
Monitoring your vision
If you have been diagnosed with dry AMD, you should use a chart called an Amsler grid every day to monitor your vision, as dry AMD can change into the more damaging wet form.
To use the Amsler grid, wear your reading glasses and hold the grid 12 to 15 inches away from your face in good light.
- Cover one eye.
- Look directly at the center dot with the uncovered eye and keep your eye focused on it.
- While looking directly at the center dot, note whether all lines of the grid are straight or if any areas are distorted, blurry or dark.
- Repeat this procedure with the other eye.
- If any area of the grid looks wavy, blurred or dark, contact your ophthalmologist immediately.
If you detect any changes when looking at the grid, you should notify your ophthalmologist immediately.
Wet, or exudative, AMD (also called neovascular AMD)
The wet form of macular degeneration occurs in about 10 percent of all macular degeneration cases, but it can cause more damage to your central or detail vision than the dry form.
Capillaries, or tiny blood vessels, extend into all tissues of the body, bringing in nutrients and carrying off waste products. Capillaries usually don’t increase in size or number, but if they do, it is called abnormal blood vessel growth.
Wet AMD occurs when abnormal blood vessels begin to grow underneath the retina. This blood vessel growth is called choroidal neovascularization (CNV) because these vessels grow from the layer under the retina called the choroid. These new blood vessels may leak fluid or blood, blurring or distorting central vision. Vision loss from this form of AMD may be faster and more noticeable than that from dry AMD.
The longer these abnormal vessels leak or grow, the more risk you have of losing more of your detailed vision. Also, if abnormal blood vessel growth happens in one eye, there is a risk that it will occur in the other eye. The earlier that wet AMD is diagnosed, the better chance you have of preserving some or much of your central vision. That is why it is so important that you and your monitor your vision in each eye carefully.
In its earliest stages, macular degeneration may cause the following symptoms:
- Blurry distance and/or reading vision;
- Distorted vision — straight lines will appear bent, crooked or irregular;
- Dark gray spots or blank spots in your vision;
- Size of objects may appear different for each eye;
- Colors do not look the same for each eye.
Doctors and researchers don't know the exact causes of AMD but it is clear that this disease is strongly associated with age, since AMD occurs as people grow older. One large study found that the risk of getting AMD jumps from about 2 percent of middle-aged people in their 50s to nearly 30 percent in people over age 75.
Our bodies constantly react with the oxygen in our environment. Over our lifetimes, as a result of this activity, our bodies produce tiny molecules called free radicals. These free radicals affect our cells, sometimes damaging them. This is called oxidative stress and is thought to play a major role in how AMD develops.
Heredity is another risk factor for AMD. People who have a close family member with the disease have a greater chance of developing AMD themselves.
Some studies have shown that inflammation (swelling of the body’s tissues) may play a role in AMD development. Inflammation is the way the body’s immune system fights off infection or other things it considers “invaders.” But an overactive immune system with its associated inflammation may be a risk factor for AMD.
Smoking and high blood pressure are associated with the wet form of AMD. Research also suggests there may be a link between being obese and having early or intermediate-stage AMD develop into advanced (wet) AMD.
Many older people develop macular degeneration as part of the body’s natural aging process. Approximately 1 in 3 Caucasians have genetic changes that make them more prone to damage from oxidative stress, when certain molecules affect our cells, which can lead to AMD.
Major risk factors for AMD are:
- Being older than 50 years old;
- Having a family history of AMD;
- Cigarette smoking.
Another risk factor for developing AMD may include having abnormal cholesterol levels or having high blood pressure (called hypertension).
Many people do not realize they have a macular problem until they notice they have blurred or distorted vision. Regular eye examinations by an ophthalmologist may help to detect problems before you are even aware of them. Your ophthalmologist can see early stages of AMD during a comprehensive eye examination.
The American Academy of Ophthalmology recommends that adults with no signs or risk factors for eye disease get a baseline eye disease screening at age 40 — the time when early signs of disease and changes in vision may start to occur. Based on the results of the initial screening, an ophthalmologist will prescribe the necessary intervals for follow-up exams.
To check for macular degeneration, your eye doctor will dilate (widen) your pupils using eyedrops and examine your eyes with an ophthalmoscope, a device that allows him or her to see the retina and other areas at the back of the eye. If AMD is detected, your doctor may have you use an Amsler grid to check for wavy, blurry or dark areas in your vision.
Fluorescein angiography
If your ophthalmologist finds an abnormality during an exam and suspects the wet form of AMD, he or she will take special photographs of your eye called fluorescein angiography. These photographs determine if abnormal blood vessels are under the retina.
To do this test, fluorescein dye is injected into a vein in your arm. The dye travels throughout the body, including your eyes. Photographs are taken of your eye as the dye passes through the retinal blood vessels. Abnormal areas will be highlighted by the dye, indicating to your doctor whether treatment is possible. If treatment options are available, these photographs will provide your doctor with a map to guide the treatment.
Unfortunately, at this time there is no single proven treatment for the dry form of AMD. However, a large scientific study has shown that antioxidant vitamins and zinc may reduce the impact of AMD in some people by slowing its progression toward more advanced stages.
The Age-Related Eye Disease Study (AREDS) showed that among people at high risk for developing late-stage, or wet, AMD (such as those who have large amounts of drusen or who have significant vision loss in at least one eye), taking a dietary supplement of vitamin C, vitamin E and beta carotene, along with zinc, lowered the risk of AMD progressing to advanced stages by about 25 percent. The daily supplements also reduced the risk of vision loss for those at risk by about 19 percent. The supplements did not appear to provide a benefit for people with minimal AMD or people without evidence of AMD during the course of the study.
The AREDS nutrient supplementation shown to be beneficial includes:
- Vitamin C – 500 mg
- Vitamin E – 400 IU
- Beta carotene – 15 mg (25,000 IU)
- Zinc oxide – 80 mg
- Copper (as cupric oxide) – 2 mg (to prevent copper deficiency, which may be associated with taking high amounts of zinc)
Another large study in women showed a benefit from taking folic acid and vitamins B6 and B12. And a large study evaluating the possible benefits of lutein and fish oil (omega-3) is ongoing.
These vitamins and minerals are recommended in specific daily amounts in addition to a healthy, balanced diet. Some people may not wish to take large doses of antioxidants or zinc because of medical reasons. Beta carotene has been shown to increase the risk of lung cancer in smokers or recent past smokers, so this supplement should not be used by people who currently smoke or recently quit smoking.
It is very important to remember that vitamin supplements are not a cure for AMD, nor will they give you back vision that you may have already lost from the disease. However, specific amounts of these supplements do play a key role in helping some people at high risk for developing advanced (wet) AMD to maintain their vision. Talk with your ophthalmologist to find out if you are at risk for developing advanced AMD, and to learn if supplements are recommended for you.
Treating wet AMD
Treating the wet form of AMD may involve the use of anti-VEGF treatment, thermal laser treatment or photodynamic therapy (PDT). Treatment of wet AMD generally reduces the risk of severe vision loss, but it does not eliminate this risk.
Anti-VEGF treatment
A common way to treat wet AMD targets a specific chemical in your body that causes abnormal blood vessels to grow under the retina. That chemical is called vascular endothelial growth factor, or VEGF. Several new drugs (called anti-VEGF drugs) have been developed that can block the trouble-causing VEGF. Blocking VEGF reduces the growth of abnormal blood vessels, slows their leakage, helps to slow vision loss, and in some cases improves vision.
Your ophthalmologist administers the anti-VEGF drug directly to your eye in an outpatient procedure. Before the procedure, your ophthalmologist will clean your eye to prevent infection and will use an anesthetic to numb your eye with a very fine needle. You may receive multiple anti-VEGF injections over the course of many months.
In some cases, your ophthalmologist may recommend combining anti-VEGF treatment with other therapies. The treatment that’s right for you will depend on the specific condition of your macular degeneration.
Thermal laser treatment
Another form of treatment for wet AMD is with thermal laser therapy. Laser treatment is usually done as an outpatient procedure in the doctor’s office or at the hospital. The laser beam in this procedure is a high-energy, focused beam of light that produces a small burn when it hits the area of the retina to be treated. This destroys the abnormal blood vessels, preventing further leakage, bleeding and growth.
Following laser treatment, vision may be more blurred than before treatment, but often it will stabilize within a few weeks. A scar forms where the treatment occurred, creating a permanent blind spot that might be noticeable in your field of vision.
Usually the abnormal blood vessels are destroyed by laser treatment. However, it is likely that 50 percent of patients with wet AMD who receive this laser procedure will need a re-treatment within three to five years. You may be instructed to use the Amsler grid daily to monitor your vision for signs of change.
Photodynamic therapy (PDT)
In some cases, a type of treatment for wet AMD called photodynamic therapy, or PDT, may be an option.
This therapeutic procedure uses a combination of a light-activated drug called a photosensitizer and a special low-power, or cool, laser to treat wet AMD right at the center of the macula.
This procedure is done on an outpatient basis, usually in an ophthalmologist’s office. The photosensitive drug is injected into a vein in your arm, where it travels through the body, including the abnormal vessels behind the central macula. The low-power laser light is targeted directly on the abnormal vessels, activating the drug, which causes damage specifically to those unwanted blood vessels.
After PDT, the abnormal blood vessels may reopen, so multiple treatments may be required.
It is important to remember that only about 10 percent of all AMD cases are exudative, or wet form, and about 75 percent of these cases cannot be treated. People with wet or dry AMD who cannot be treated will not become blind, as they will still have peripheral, or side, vision.
If you have untreatable AMD, you can make the most of your remaining vision by learning to “see again” with the vision you do have and with the help of special low-vision rehabilitation, devices and services. People with low vision can learn new strategies to accomplish daily activities. These skills, including mastering new techniques and devices, help people with advanced AMD regain their confidence and live independently despite loss of central vision.
While there is little that can be done to improve the eyesight of someone who has AMD, with early detection, the rate of vision loss can be slowed. The keys to slowing vision loss are to understand your condition and work closely with your ophthalmologist to monitor your vision. Even with macular degeneration, you can still maintain an enjoyable lifestyle.
Vision rehabilitation
Vision rehabilitation can help people with low vision compensate for vision loss. People with low vision can learn new strategies to accomplish daily activities. These skills, including mastering new techniques and devices, help people with advanced vision loss regain their confidence and live independently.
How much rehabilitation is needed depends on your vision loss and what you want to be able to do. A team approach is often best and may involve some or all of the following professionals: ophthalmologist, low-vision specialist, occupational therapist, rehabilitation teacher, orientation and mobility specialist, social worker and counselor.
This rehabilitation process can be a challenging and frustrating period of adjustment — one that requires patience, practice, motivation and the support of your doctor, low-vision specialist, family and friends. The rewards, however, can be great.
Low-vision aids
There are many devices specifically designed to help people with low vision function better. Different devices are available for different tasks. A trained professional can help you understand which device is best for accomplishing your particular needs. Training and practice are also important in order to become skilled at using any device.
Optical low-vision devices
Optical low-vision devices use lenses to magnify objects, making them easier to see. The lens strength will depend on your vision and the size of the object or print to be seen.
- Magnifying spectacles. Stronger than ordinary glasses. They can be used for near tasks, such as reading, threading a needle, or any activity that requires detailed vision. The printed page or object must be held closer than usual in order to keep things in focus. One advantage of magnifying spectacles is that your hands remain free to hold reading materials or perform tasks.
- Hand magnifiers. Familiar to most people and are available in varying strengths. Reading material is not necessarily held as close to the face as with magnifying spectacles, and some models come with a built-in light. High-quality and high-powered magnifiers are often available only in specialized stores or through vision rehabilitation professionals.
- Stand magnifiers. Rest directly on the reading material, keeping the lens at the proper distance from the page. The ability to rest the magnifier on the page is useful for patients with a tremor or arthritis.
- Telescopes. Used for seeing objects or reading signs that are far away. They can be handheld like a pair of regular binoculars or mounted on a pair of eyeglasses.
- Video magnifiers. Electronic devices that use a camera and television screen to enlarge printed material, pictures, or small objects. They are adjustable and can enhance the material in different ways — for example, by making the print appear darker (increased contrast). The technology is developing rapidly, and electronic devices are becoming smaller, more portable and easier to use. Some can even be used for both distance and near tasks.
Other low-vision devices and techniques
There are numerous low vision aids, devices, and techniques to help make everyday activities easier. They include:
- Large-print books, newspapers, magazines, playing cards, and banking checks; high-contrast and large number telephones, thermostats, watches, and remote controls; talking watches, timers, books, and medical devices;
- Bold-tipped markers for easy-to-read shopping and phone number lists;
- Computers that can magnify (on screen or on paper) any printed material or picture, or that read aloud what is viewed on screen;
- Sitting closer to the television. (This will not damage your eyes.)
Lighting and glare
Good lighting and glare control are very important for people with low vision. A bright light should always be used when reading and its location should be adjusted for the greatest visibility without glare. Stronger light bulbs in darkly lit areas can make tasks like cooking, dressing, and walking up and down stairs easier. Wearing a hat with a wide brim or tinted wraparound sunglasses can shield your eyes from dazzling and annoying overhead lights or sunlight.
If your vision has become cloudy or things you see are not as bright as they used to be, a cataract may have developed in one or both of your eyes. A cataract is a clouding of the eye’s naturally clear lens. Your eye becomes like a window that is frosted or yellowed.
The amount and pattern of cloudiness within the lens can vary. If the cloudiness is not near the center of the lens, you may not be aware that a cataract is present.
There are many misconceptions about cataract. A cataract is not:
- A growth or film over the eye;
- A cause of irreversible blindness;
- A result of overusing the eyes;
- A contagious disease spread from eye to eye or person to person.
Cataracts are a common cause of vision loss, especially as we age, but they are treatable. Your eye doctor can tell you whether cataract or some other problem is the cause of your vision loss and can help you decide if cataract surgery is appropriate for you.

Above: Dulled or yellowed vision from cataracts.

Above: Blurring or dimming vision from cataracts.

Above: Distortion or ghost images from cataracts.
The only way to know if you have cataracts for certain is when your ophthalmologist (Eye M.D.) does a dilated eye exam. Get a baseline exam at age 40, when early signs of disease and changes in vision may start to occur. Your Eye M.D. will let you know how often you should return for follow-up exams. At any point, if you have symptoms or risks for eye disease, see your Eye M.D. Because your risk for cataracts and other eye diseases increases as you get older, starting at age 65 you should see your Eye M.D. every year. A complete eye examination will rule out any other condition that may be causing blurred vision or eye problems.
Most age-related cataracts develop gradually. As a result, you may not immediately notice changes in your vision when cataracts first develop.
In time, you may have symptoms such as:
- Painless clouded, blurry or dim vision;
- Increasing difficulty seeing at night or in low light;
- Sensitivity to light and glare, seeing halos around lights;
- Colors seem faded or yellowed;
- The need for brighter light for reading and other activities;
- Frequent changes in eyeglass or contact lens prescription; or
- Double vision within one eye.
If you detect any changes when looking at the grid, you should notify your ophthalmologist immediately.
Cataracts occur as part of the aging process, so everyone is at risk eventually. By age 75, about 70 percent of people will have cataracts. The eye’s lens slowly becomes less flexible, less transparent and thicker. Then areas of the lens become cloudy. Usually cataracts develop in both eyes at about the same time.
These factors increase the risk of developing cataracts:
- Advanced age;
- Diabetes;
- Family history;
- Smoking;
- Previous eye injury or inflammation;
- Prolonged steroid use (especially combined use of oral and inhaled steroids); and
- Extensive exposure to sunlight.
If you have any of these risk factors, you should schedule an appointment with your ophthalmologist
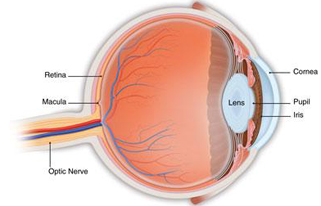
The design of the human eye is much like that of a camera. Light rays are focused through the lens onto the retina, a layer of light-sensitive cells at the back of the eye that is similar to film. In a normal eye, light rays pass through a clear lens and are focused onto the retina. This produces a bright, clear image.
As the body ages, the lens continues to grow layers onto the existing surface. Over time the lens hardens and becomes cloudy, which often results in dull, cloudy or blurred vision. This condition, known as an age-related cataract, is normal and occurs eventually in most people.
If the clouding is mild or affects only a small area of the lens, your vision may be only slightly affected. If there is more clouding and it affects the entire lens, your vision will become severely limited.
Less common types of cataracts, not related to normal aging, include:
- Congenital or developmental cataracts: Can occur in children. They may be hereditary or can be associated with some birth defects. Some occur without any obvious cause.
- Secondary cataracts: Caused by other eye diseases or previous surgery within the eye. Formation of secondary cataracts may be accelerated by a chronic disease, such as diabetes, or excessive use of steroid medications.
- Traumatic cataracts: Related directly to an eye injury. Traumatic cataracts may appear immediately following injury, or develop several months or even years later.
During a comprehensive, dilated eye exam, your Eye M.D. uses several tests to check for cataracts:
- Slit-lamp: This device allows your Eye M.D. to closely examine the eye’s cornea, iris, lens and the space between the iris and cornea. The doctor is able to examine the eye in small sections, making it easier to see abnormalities.
- Retinal exam: When your eye is dilated, the pupils are wide open so the doctor can more clearly see the back of the eye. Using the slit lamp and/or an instrument called an ophthalmoscope, the doctor looks for signs of cataract and if present, the extent of the clouding. Your Eye M.D. will also look for signs of glaucoma and other potential problems with the retina and optic nerve.
- : Related directly to an eye injury. Traumatic cataracts may appear immediately following injury, or develop several months or even years later.
- Have an eye exam every year if you’re older than 65, or every two years if younger.
- Protect your eyes from UV light by wearing sunglasses that block at least 99 percent UV and a hat.
- If you smoke, quit; smoking can increase cataract progression.
- Use brighter lights for reading and other activities; a magnifying glass may be useful, too.
- Limit night driving once night vision, halos or glare become problems.
- Take care of any other health problems, especially diabetes.
- Get the right eyeglasses or contact lenses to correct your vision; when it becomes too difficult to complete your regular activities, consider cataract surgery.
Do not use eyedrops or other treatments that claim to dissolve or remove cataracts. There is no proven way to dissolve cataracts with eyedrops. Surgery is the only way to remove cataracts.
If your vision is only slightly blurry, a change in your eyeglass prescription may help for a while. However, if you are still not able to see well enough to do the things you like or need to do after the change in eyeglass prescription, cataract surgery should be considered.
Cataract surgery is often performed as an outpatient procedure and does not require an overnight stay. There are usually few restrictions, and you will be able to resume your normal activities almost immediately.
Before surgery, the length of your eye will be measured in what is called an A-scan, and the curve of your cornea will be measured in a technique called keratometry. These measurements help your Eye M.D. select the proper lens implant for your eye.
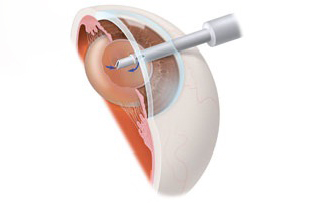
The most common procedure used for removing cataracts is called phacoemulsification. A small incision is made in the side of the cornea (the front part of your eye). Your Eye M.D. inserts a tiny instrument through the incision that uses high-frequency ultrasound to break up the center of the cloudy lens and suction it out. The lens is removed in one piece, using a technique called extracapsular extraction.
After the cloudy lens has been removed, the surgeon will replace it with an intraocular lens implant made of plastic, silicone or acrylic. This new lens allows light to pass through and focus on the retina. The IOL becomes a permanent part of your eye. In most cases, the IOL is inserted behind the iris, the colored part of your eye, and is called a posterior chamber lens. Sometimes, the IOL must be placed in front of the iris. This is called an anterior chamber lens. When the IOL is in place, the surgeon closes the incision. Stitches may or may not be used.
In some cases, the part of the lens covering that supports the IOL (called the capsule) can become cloudy several months or years after the first cataract was removed. This is called an “after cataract” or “secondary cataract.” If this occurs and blurs your vision, your Eye M.D. will make an opening in the center of the cloudy capsule with a laser to allow light to pass through the lens properly again. This procedure, called a posterior capsulotomy, takes about five minutes in the doctor’s office and requires no recovery period.
If you are having cataract surgery, be sure to tell your doctor if you are currently or have ever used alpha-blocker medications such as Flomax®, Uroxatral® or Cadura®. These medications affect the iris or pupil and can lead to complications during cataract surgery. You can still have a successful surgery if your surgeon knows that you have taken these drugs and appropriately adapts his or her surgical technique. You should also tell your Eye M.D. about any other sedative medications you are taking.
Also, if you plan to have cataract surgery and you have had LASIK or other laser refractive surgery, provide your Eye M.D. with the vision correction prescription you had before LASIK, if possible. This information will help your Eye M.D. calculate the correct IOL prescription for you.
Most people who wear bifocals or reading glasses for near vision may still need to wear glasses after cataract surgery for reading, and, in some cases, even for distance. If you choose to have a multifocal or accommodative IOL, your dependence on glasses may be minimized or, in some cases, eliminated completely.
Before intraocular lenses (IOLs) were developed, people had to wear very thick eyeglasses or special contact lenses to be able to see after cataract surgery. Today several IOL types are available to help people enjoy improved vision. Discuss these options with your Eye M.D. to determine the IOL that best suits your vision needs and lifestyle.
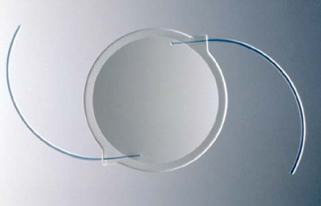
Like your eye’s natural lens an IOL focuses light as images, received from the cornea and pupil at the front of the eye, onto the retina, the sensitive tissue at the back of the eye that relays images through the optic nerve to the brain. Most IOLs are made of a flexible, foldable material and are about one-third of the size of a dime. Like the lenses of prescription eyeglasses, your IOL will contain the appropriate prescription to give you the best vision possible. Read below to learn about how IOL types correct specific vision problems.

- Before surgery your eyes are measured to determine your IOL prescription, and you and your Eye M.D. decide which IOL type will be best for you, in part depending on how you feel about wearing glasses for reading and near vision.
- The type of IOL implanted will affect how you see when not wearing eyeglasses. Glasses may still be needed by some people for some activities.
- If you have astigmatism your Eye M.D. will discuss toric IOLs and related treatment options with you.

Monofocal: This IOL type has been in use for several decades.
- Monofocals are set to provide best corrected vision at near, intermediate or far distances.
- Most people who choose monofocals have their IOLs set for distance vision and use reading glasses for near activities. On the other hand, a person whose IOLs were set to correct near vision would need glasses to see distant objects clearly.
- Some who choose monofocals decide to have the IOL for one eye set for distance vision, and the other set for near vision, a strategy called “monovision.” The brain adapts and synthesizes the information from both eyes to provide vision at intermediate distances. Often this reduces the need for reading glasses. People who regularly use computers, PDAs or other digital devices may find this especially useful. Individuals considering monovision may have a trial with monovision contact lenses to learn how well they can adapt to monovision. Those who require crisp, detailed vision may decide monovision is not for them. People with appropriate vision prescriptions may find that monovision allows them see well at most distances with little or no need for eyeglasses.
- Presbyopia is a condition that affects everyone at some point after age 40, when the eye’s lens becomes less flexible and makes near vision more difficult, especially in low light. Since presbyopia makes it difficult to see near objects clearly, even people without cataracts need reading glasses or an equivalent form of vision correction.

Multifocal or accommodative:: These newer IOL types reduce or eliminate the need for glasses or contact lenses.
- In the multifocal type, a series of focal zones or rings is designed into the IOL. Depending on where incoming light focuses through the zones, the person may be able to see both near and distant objects clearly.
- The design of the accommodative lens allows the eye’s ciliary muscles to move the IOL forward and backward, thus allowing the focus to change much as it would with a natural lens and enabling near and distance vision.
- The ability to read and perform other tasks without glasses varies from person to person but is generally best when multifocal or accommodative IOLs are placed in both eyes.
- Usually 6 to 12 weeks are required after surgery on the second eye for the brain to adapt and for full visual improvement to be realized with either of these IOL types.
Considerations with multifocal or accommodative IOLs
- For many people, these IOL types reduce but do not eliminate the need for glasses or contact lenses. For example, a person can read without glasses, but the words appear less clear than with glasses.
- The effectiveness in a specific person may depend on the size of his/her pupils and other eye health factors. People with astigmatism can ask their Eye M.D. about toric IOLs and related treatments
- Side effects such as glare or halos around lights, or decreased sharpness of vision (contrast sensitivity) may occur, especially at night or in dim light. Most people adapt and are not bothered by these effects, but those who frequently drive at night or need to focus on close-up work may be more satisfied with monofocal IOLs.
Toric: This is a monofocal IOL with astigmatism correction built into the lens.
- Astigmatism: This eye condition distorts or blurs the ability to see both near and distant objects. With astigmatism the cornea (the clear front window of the eye) is not round and smooth (like a basketball), but instead is curved like a football. People with significant degrees of astigmatism are usually most satisfied with toric IOLs.
- People who want to reduce (or possibly eliminate) the need for eyeglasses may opt for an additional treatment called limbal relaxing incisions, which may be done at the same time as cataract surgery or separately. These small incisions allow the cornea’s shape to be rounder or more symmetrical.
Protective filters:IOLs include filters to protect the eye’s retina from exposure to UV and other potentially damaging light radiation. The Eye M.D. selects the filters that will provide appropriate protection for the patient’s specific needs.
Other important considerations
- If, after healing completely from the initial cataract removal and IOL implantation, a person needs further correction to achieve the best vision possible, the Eye M.D. may recommend additional surgery to exchange an IOL for another type, implant an additional IOL, or make limbal relaxing incisions in the cornea. Other laser refractive surgery may be recommended in some cases.
- People who have had previous refractive surgery such as LASIK need to be especially carefully evaluated before receiving IOLs because the ability to calculate the correct IOL prescription (PDF 650K) may be affected by the previous refractive surgery.
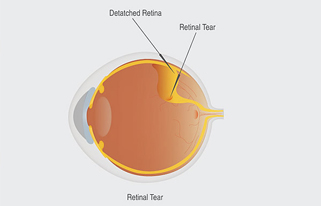
Eye illustration which shows a retinal tear, fluid behind the retina and a detached retina.
Usually the vitreous moves away from the retina without causing problems. But sometimes the vitreous pulls hard enough to tear the retina in one or more places. Fluid may pass through a retinal tear, lifting the retina off the back of the eye — much as wallpaper can peel off a wall. When the retina is pulled away from the back of the eye like this, it is called a retinal detachment.
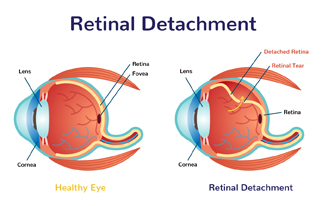
The retina is the light-sensitive tissue lining the back of our eye. Light rays are focused onto the retina through our cornea, pupil and lens. The retina converts the light rays into impulses that travel through the optic nerve to our brain, where they are interpreted as the images we see.
The middle of our eye is filled with a clear gel called vitreous (vit-ree-us) that is attached to the retina.
Sometimes tiny clumps of gel or cells inside the vitreous will cast shadows on the retina, and you may sometimes see small dots, specks, strings or clouds moving in your field of vision. These are called floaters. You can often see them when looking at a plain, light background, like a blank wall or blue sky.
As we get older, the vitreous may shrink and pull on the retina. When this happens, you may notice what look like flashing lights, lightning streaks or the sensation of seeing “stars.” These are called flashes.
Usually the vitreous moves away from the retina without causing problems. But sometimes the vitreous pulls hard enough to tear the retina in one or more places. Fluid may pass through a retinal tear, lifting the retina off the back of the eye — much as wallpaper can peel off a wall. When the retina is pulled away from the back of the eye like this, it is called a retinal detachment.
The retina does not work when it is detached and vision is blurry. A retinal detachment is a very serious problem that almost always causes blindness unless it is treated.
People with the following conditions have an increased risk for retinal detachment:
- Nearsightedness;
- Previous cataract surgery;
- Glaucoma;
- Severe eye injury;
- Previous retinal detachment in the other eye;
- Family history of retinal detachment;
Weak areas in the retina that can be seen by an ophthalmologist.
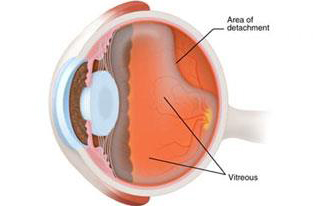
The middle of the eye is filled with a clear gel called vitreous (vit-ree-us) that is attached to the retina. As we get older, the vitreous may shrink and pull away from the retina.
Usually the vitreous separates from the retina without causing problems. But sometimes the vitreous pulls hard enough to tear the retina in one or more places. Fluid may pass through the retinal tear, lifting the retina off the back of the eye, much as wallpaper can peel off a wall.

Your ophthalmologist can diagnose retinal tear or detachment during an eye examination where he or she dilates (widens) the pupils of your eyes. Some retinal detachments are found during a routine eye examination.
Only after careful examination can your ophthalmologist tell whether a retinal tear or early retinal detachment is present.
Retinal tears
Most retinal tears need to be treated by sealing the retina to the back wall of the eye with laser surgery or cryotherapy (a freezing treatment). Both of these procedures create a scar that helps seal the retina to the back of the eye. This prevents fluid from traveling through the tear and under the retina, which usually prevents the retina from detaching. These treatments cause little or no discomfort and may be performed in your ophthalmologist’s office.
Retinal detachments
Almost all patients with retinal detachments must have surgery to place the retina back in its proper position. Otherwise, the retina will lose the ability to function, possibly permanently, and blindness can result. The method for fixing retinal detachment depends on the characteristics of the detachment. In each of the following methods, your Eye M.D. will locate the retinal tears and use laser surgery or cryotherapy to seal the tear.
Scleral buckle
This treatment involves placing a flexible band (scleral buckle) around the eye to counteract the force pulling the retina out of place.The ophthalmologist often drains the fluid under the detached retina, allowing the retina to settle back into its normal position against the back wall of the eye. This procedure is performed in an operating room.
Pneumatic retinopexy
In this procedure, a gas bubble is injected into the vitreous space inside the eye in combination with laser surgery or cryotherapy. The gas bubble pushes the retinal tear into place against the back wall of the eye. Sometimes this procedure can be done in the ophthalmologist’s office. Your ophthalmologist will ask you to constantly maintain a certain head position for several days. The gas bubble will gradually disappear.
Vitrectomy
This surgery is performed in an operating room. The vitreous gel, which is pulling on the retina, is removed from the eye and usually replaced with a gas bubble. Your body’s own fluids will gradually replace the gas bubble. Sometimes vitrectomy is combined with a scleral buckle.
Most retinal detachment surgery is successful, although a second operation is sometimes needed.
Some retinal detachments cannot be fixed. If the retina cannot be reattached, the eye will continue to lose sight and ultimately become blind.
After successful surgery for retinal detachment, vision may take many months to improve and, in some cases, may never return fully. Unfortunately, some patients do not recover any vision. The more severe the detachment, the less vision may return. For this reason, it is very important to see your ophthalmologist at the first sign of any trouble.
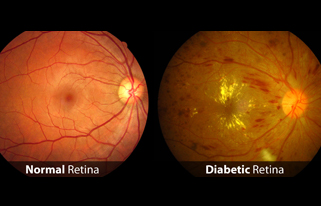
Diabetic retinopathy, the most common diabetic eye disease, is caused by changes in the blood vessels of the retina.
There are two types of diabetic retinopathy:
- Background or nonproliferative diabetic retinopathy (NPDR); and
- Proliferative diabetic retinopathy (PDR).
Nonproliferative diabetic retinopathy (NPDR)
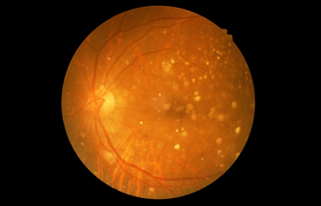
Nonproliferative diabetic retinopathy (NPDR) is the earliest stage of diabetic retinopathy. With this condition, damaged blood vessels in the retina begin to leak extra fluid and small amounts of blood into the eye. Sometimes, deposits of cholesterol or other fats from the blood may leak into the retina.
NPDR can cause changes in the eye, including:
- Microaneurysms Small bulges in blood vessels of the retina that often leak fluid.
- Retinal hemorrhagesTiny spots of blood that leak into the retina (these spots alone are rarely responsible for any loss of vision).
- Hard exudates Deposits of cholesterol or other fats from the blood that have leaked into the retina.Many people with diabetes have mild NPDR, which usually does not affect their vision. However, if their vision is affected, it is the result of macular edema and macular ischemia.
- Macular edema Swelling or thickening of the macula. It is caused by fluid leaking from the retina’s blood vessels. The macula, which is responsible for our clear, central vision, does not function properly when it is swollen. Macular edema is the most common cause of vision loss in diabetes. Vision loss may be mild to severe, but in many cases, your peripheral (side) vision remains. Laser treatment may help to stabilize vision.
- Macular ischemia Occurs when small blood vessels (capillaries) close. Your vision blurs because the macula no longer receives enough blood to work properly. Currently, there is no effective treatment for macular ischemia.
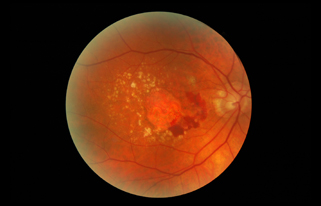
Proliferative diabetic retinopathy (PDR)
Proliferative diabetic retinopathy (PDR) occurs when abnormal blood vessels begin to grow on the surface of the retina or optic nerve. This is called neovascularization. PDR mainly occurs when many of the blood vessels in the retina close, preventing enough blood flow. The retina responds by growing new blood vessels in an attempt to supply the area where the original vessels closed. However, the new blood vessels are abnormal and do not supply the retina with normal blood flow. The new vessels are also often accompanied by scar tissue that may cause the retina to wrinkle or detach.
PDR may cause more severe vision loss than NPDR because it can affect both central and peripheral vision.
PDR causes vision loss in the following ways:
- Vitreous hemorrhage The delicate new blood vessels may bleed into the vitreous — the gel in the center of the eye — preventing light rays from reaching the retina. If the vitreous hemorrhage is small, you may see a few new, dark floaters. A very large hemorrhage might block out all vision, allowing you to perceive only light and dark. Vitreous hemorrhage alone does not cause permanent vision loss. When the blood clears, your vision may return to its former level unless the macula has been damaged.
- Traction retinal detachment With PDR, scar tissue from neovascularization can shrink, causing the retina to wrinkle and pull from its normal position. This is called traction retinal detachment. Macular wrinkling can distort your vision. More severe vision loss can occur if the macula or large areas of the retina are detached.
- Neovascular glaucoma Occasionally, if a number of retinal vessels are closed, neovascularization can occur in the iris (the colored part of the eye). In this condition, the new blood vessels may block the normal flow of fluid out of the eye. Pressure builds up in the eye, resulting in neovascular glaucoma, a particularly severe eye disease that causes damage to the optic nerve.
Diabetes can cause vision in both eyes to change, even if you do not have retinopathy. Rapid changes in your blood sugar alter the shape of your eye’s lens, and the image on the retina will become out of focus. After your blood sugar stabilizes, the image will be back in focus. You can reduce episodes of blurred vision by maintaining good control of your blood sugar.

Diabetic retinopathy usually takes years to develop, which is why it is important to have regular eye exams. Because people with Type 2 diabetes may have been living with the disease for some time before they are diagnosed, it is important that they see ophthalmologist without delay. The American Academy of Ophthalmology recommends the following schedule for people with diabetes:
- Type 1: Within five years of being diagnosed and then yearly.
- Type 2: At the time of diabetes diagnosis and then yearly.
- During pregnancy: Pregnant women with diabetes should schedule an appointment with their ophthalmologist in the first trimester because retinopathy can progress quickly during pregnancy.
Diabetes is a disease that affects the body’s ability to produce and/or use insulin in amounts sufficient to control blood sugar levels. There are three types of diabetes: type 1, type 2 and gestational, which may develop when a woman is pregnant.
- Type 1 Usually diagnosed in children and young adults and previously known as juvenile diabetes. The body does not produce insulin.
- Type 2 The most common form of diabetes. Either the body does not produce enough insulin or the body’s cells ignore the insulin.
- Gestational Blood sugar levels (glucose) become elevated during pregnancy in women who have never had diabetes before. Gestational diabetes starts when the mother’s body is not able to make and use all the insulin it needs during pregnancy.
People with any type of diabetes can develop hyperglycemia, which is an excess of blood sugar, or serum glucose. Although glucose is a vital source of energy for the body’s cells, a chronic elevation of serum glucose causes damage throughout the body, including the small blood vessels in the eyes.
As a result, if you have diabetes you run the risk of developing diabetic retinopathy, in which damage occurs to the delicate blood vessels inside the retina at the back of the eye. You are also at increased risk for developing cataracts (clouding of the normally clear lens in the eye), or glaucoma (a disease that results in damage to the optic nerve). However, with an annual dilated eye exam and control of blood sugar levels, 90 percent of vision loss can be avoided.
Diabetic retinopathy risk factors
Several factors can influence the development and severity of diabetic retinopathy, including:
- Blood sugar levels Controlling your blood sugar is the key risk factor that you can affect. Lower blood sugar levels can delay the onset and slow the progression of diabetic retinopathy.
- Blood pressure A major clinical trial demonstrated that effectively controlling blood pressure reduces the risk of retinopathy progression and visual acuity deterioration. High blood pressure damages your blood vessels, raising the chances for eye problems. Target blood pressure for most people with diabetes is less than 130/80 mmHg.
- Duration of diabetes The risk of developing diabetic retinopathy or having your disease progress increases over time. After 15 years, 80 percent of Type 1 patients will have diabetic retinopathy. After 19 years, up to 84 percent of patients with Type 2 diabetes will have diabetic retinopathy.
- Blood lipid levels (cholesterol and triglycerides) Elevated blood lipid levels can lead to greater accumulation of exudates, protein deposits that leak into the retina. This condition is associated with a higher risk of moderate visual loss.
- Ethnicity While diabetic retinopathy can happen to anyone with diabetes, certain ethnic groups are at higher risk because they are more likely to have diabetes. These include African Americans, Latinos and Native Americans.
- Pregnancy Being pregnant can cause changes to your eyes. If you have diabetes and become pregnant, your risk for diabetic retinopathy increases. If you already have diabetic retinopathy, it may progress. However, some studies have suggested that with treatment these changes are reversed after you give birth and that there is no increase in long-term progression of the disease
The best treatment is to prevent the development of retinopathy. Strict control of your blood sugar will significantly reduce the long-term risk of vision loss. Treatment will not usually cure diabetic retinopathy or restore normal visual acuity, but it may slow the progression of visual loss. Without treatment, diabetic retinopathy progresses steadily from minimal to severe stages.
Laser surgery
The laser is a very bright, finely focused light. It passes through the clear cornea, lens and vitreous without affecting them in any way. Laser surgery shrinks abnormal new vessels and reduces macular swelling. Treatment is often recommended for people with macular edema, proliferative diabetic retinopathy (PDR) and neovascular glaucoma.
Laser surgery is usually performed in an office setting. For comfort during the procedure, an anesthetic eyedrop is often all that is necessary, although an anesthetic injection is sometimes given next to the eye. The patient sits at an instrument called a slit-lamp microscope. A contact lens is temporarily placed on the eye in order to focus the laser light on the retina with pinpoint accuracy.
For macular edema, the laser is applied near the macula in order to reduce fluid leakage. The main goal of treatment is to prevent further loss of vision by reducing the swelling of the macula. It is uncommon for people who have blurred vision from macular edema to recover normal vision, although some will experience partial improvement. A few people may see laser spots near the center of their vision following treatment. They usually fade with time, but may not disappear completely.
In PDR, the laser is applied to all parts of the retina except the macula (called PRP, or panretinal photocoagulation). This treatment causes abnormal new vessels to shrink and often prevents them from growing in the future. It also decreases the chance that vitreous bleeding or retinal distortion will occur. Panretinal laser has proven to be very effective for preventing severe vision loss from vitreous hemorrhage and traction retinal detachment.
Side effects of panretinal laser surgery may include:
- Temporary blurred vision for days to a few weeks;
- Occasional mild loss of central vision;Mild to moderate loss of peripheral vision;
- Mild to moderate loss of peripheral vision;
- Decreased night vision.
Multiple laser treatments over time may be necessary. Laser surgery does not cure diabetic retinopathy and does not always prevent further loss of vision. In spite of laser surgery, some people with PDR develop macular distortion or bleeding into the vitreous, causing blurred vision. Vitreous hemorrhage may recur and blood may accumulate faster than the eye can reabsorb it.
Vitrectomy surgery
Vitrectomy is a surgical procedure performed in a hospital or ambulatory surgery center operating room. It is often performed on an outpatient basis or with a short hospital stay. Either a local or general anesthetic may be used.
During vitrectomy surgery, an operating microscope and small surgical instruments are used to remove blood and scar tissue that accompany abnormal vessels in the eye. Removing the vitreous hemorrhage allows light rays to focus on the retina again.
Vitrectomy often prevents further vitreous hemorrhage by removing the abnormal vessels that caused the bleeding. Removal of the scar tissue helps the retina return to its normal location. Laser surgery may be performed during vitrectomy surgery. Vitrectomy surgery may be recommended for:
- Thick vitreous blood in young, insulin-dependent diabetic patients. This is because they are at high risk for traction detachment, which may be hidden behind the blood;
- Thick or repetitive vitreous hemorrhage that does not clear or significantly interferes with the person’s lifestyle;
- Recent traction detachment or distortion of the macula.
To help the retina heal in place, your ophthalmologist may place a gas bubble in the vitreous space. The gas bubble will dissolve in one to eight weeks, depending on the type of gas used. You may be told to keep your head in certain positions while the gas bubble helps to heal the retina. It is important to follow your ophthalmologist’s instructions so your eye will heal properly. You will be advised not to travel by plane or to a high altitude while this bubble is in your eye, since a rapid increase in altitude can raise your eye pressure to dangerous levels and could cause vision loss or even blindness.
Risks of vitrectomy include infection, bleeding, retinal detachment and high pressure in the eye. Cataract formation is uncommon right after surgery; however, most patients often develop a cataract after a number of months or within a few years.
Future treatments
Researchers are studying treatments that target the underlying biochemical mechanisms that cause diabetic retinopathy. One potential future treatment involves the use of VEGF inhibitors, which hinder the growth of new blood vessels. Because leakage from these abnormal blood vessels causes vision loss, preventing their growth could avoid damage to the retina.
The only way to detect diabetic retinopathy and to monitor its progression is through a comprehensive eye exam. There are several parts to the exam:
- Visual acuity test This uses an eye chart to measure how well you can distinguish object details and shape at various distances. Perfect visual acuity is 20/20 or better. Legal blindness is defined as worse than or equal to 20/200.
- Slit-lamp exam A type of microscope is used to examine the front part of the eye, including the eyelids, conjunctiva, sclera, cornea, iris, anterior chamber, lens, and also parts of the retina and optic nerve.
- Dilated exam Drops are placed in your eyes to widen, or dilate, the pupil, enabling your Eye M.D. to examine more thoroughly the retina and optic nerve for signs of damage.
It is important that your blood sugar be consistently controlled for several days when you see your eye doctor for a routine exam. If your blood sugar is uneven, causing a change in your eye’s focusing power, it will interfere with the measurements your doctor needs to make when prescribing new eyeglasses. Glasses that work well when your blood sugar is out of control will not work well when your blood sugar level is stable.
In addition to a visual acuity test and a dilated exam, your Eye M.D. may find additional tests useful.
Fluorescein angiography/optical coherence tomography (OCT)
Your doctor may order fluorescein angiography or optical coherence tomography (OCT) to further evaluate your retina or to guide laser treatment if it is necessary. Fluorescein angiography is a diagnostic procedure that uses a special camera to take a series of photographs of the retina after a small amount of yellow dye (fluorescein) is injected into a vein in your arm.
The photographs of fluorescein dye traveling throughout the retinal vessels show:
- Which blood vessels are leaking fluid;
- How much fluid is leaking;
- How many blood vessels are closed;
- Whether neovascularization is beginning.
OCT is a non-invasive scanning laser that provides high-resolution images of the retina, demonstrating its thickness. OCT can provide additional information regarding the presence and severity of macular edema.
These tests help the doctor determine:
- Why vision is blurred;
- Whether laser treatment should be started;
- Where to apply laser treatment.
Ultrasound
If your ophthalmologist cannot see the retina because of vitreous hemorrhage, an ultrasound test may be done in the office. The ultrasound can “see” through the blood to determine if your retina has detached. If there is detachment near the macula, this often calls for prompt surgery.
When the evaluation is complete, your ophthalmologist will decide when you need to be treated or re-examined.
People with diabetes should see their ophthalmologist right away if they have visual changes that:
- Affect only one eye;
- Last more than a few days;
- Are not associated with a change in blood sugar.
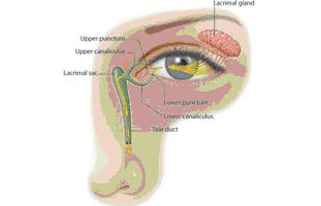
The tear film consists of three layers:
- An oily layer;
- A watery layer;
- A layer of mucus.
Each layer has its own purpose. The oily layer, produced by the meibomian glands, forms the outermost surface of the tear film. Its main purpose is to smooth the tear surface and reduce evaporation of tears.
The middle watery layer makes up most of what we ordinarily think of as tears. This layer, produced by the lacrimal glands in the eyelids, cleanses the eye and washes away foreign particles or irritants.
The inner layer consists of mucus produced by the conjunctiva. Mucus allows the watery layer to spread evenly over the surface of the eye and helps the eye remain moist. Without mucus, tears would not stick to the eye.
Normally, the eye constantly bathes itself in tears. By producing tears at a slow and steady rate, the eye stays moist and comfortable.
The eye uses two different methods to produce tears. It can make tears at a slow, steady rate to maintain normal eye lubrication. It can also produce a lot of tears in response to eye irritation or emotion. When a foreign body or dryness irritates the eye, or when a person cries, excessive tearing occurs.
It may not sound logical that dry eye would cause excess tearing, but think of it as the eye’s response to discomfort. If the tears responsible for maintaining lubrication do not keep the eye wet enough, the eye becomes irritated. Eye irritation prompts the gland that makes tears (called the lacrimal gland) to release a large volume of tears, overwhelming the tear drainage system. These excess tears then overflow from your eye.
While it may sound strange, people with dry eye may find their eyes water quite a bit. This is because the eye is responding to the irritation of this condition. Dry-eye sufferers may find that they feel like they cannot keep their eyes open for very long. They may also find their eyes feel more uncomfortable after reading or watching television.
General symptoms of dry eye usually include:
- Stinging or burning eyes;
- Scratchiness;
- Stringy mucus in or around the eyes;
- Excessive eye irritation from smoke or wind;
- Excess tearing;
- Discomfort when wearing contact lenses.
Anyone can experience dry eye, though it is more common among women, particularly after menopause. Women who experience other hormonal conditions, such as pregnancy and menstruation, may also have dry eye symptoms.
People who have a condition called Sjögren’s syndrome will usually have dry eye. So will others with similar systemic diseases like lupus or rheumatoid arthritis. Also, people who take certain over-the-counter and prescription medications can have dry eye due to reduced tear secretion.
People who have had refractive surgery, where their corneas have reduced sensation due to incisions or tissue removal, may also experience dry eye. Also, people who wear contact lenses long term are at risk for developing dry eye.
People who are sensitive to certain climates (such as windy, dry air) or to environmental factors like cigarette smoke or air conditioning may develop dry eye when they are exposed to these conditions.
Because people who work long hours at a computer are less likely to blink often, they are more susceptible to getting dry eye than people who don’t spend a lot of time in front of a computer monitor.
ormonal changes are a main cause of dry eye, causing changes in tear production. The hormonal changes associated with menopause are one of the main reasons why women are most often affected by dry eye.
Conditions that affect the lacrimal gland or its ducts — including autoimmune diseases like lupus and rheumatoid arthritis — lead to decreased tear secretion and dry eye.
Tear secretion also may be reduced by certain conditions that decrease corneal sensation. Diseases such as diabetes and herpes zoster are associated with decreased corneal sensation. So is long-term contact lens wear and surgery that involves making incisions in or removing tissue from the cornea (such as refractive surgery).
A wide variety of common medications, both prescription and over-the-counter, can cause dry eye by reducing tear secretion. Be sure to tell your ophthalmologist the names of all the medications you are taking, especially if you are using:
- Diuretics for high blood pressure;
- Beta-blockers for heart or high blood pressure;
- Antihistamines for allergies;
- Sleeping pills;
- Medications for “nerves”;
- Pain relievers.
Since these medications are often necessary, the dry eye condition may have to be tolerated or treated with eye drops called artificial tears.
People with dry eye are often more likely to experience the side effects of eye medications, including artificial tears. For example, the preservatives in certain eyedrops and artificial tear preparations can irritate the eye. These people may need special, preservative-free artificial tears.
An ophthalmologist is usually able to diagnose dry eye by examining the eyes.
Sometimes tests that measure tear production are necessary. A test called the Schirmer tear test involves placing filter-paper strips under the lower eyelids to measure the rate of tear production under various conditions.
Another diagnostic method involves putting special dye drops in the eye then studying how long it takes for dry spots to develop on the cornea. The dye test can also be used to look for certain staining patterns that show any damage to the surface of the cornea.
Adding tears
Eye drops called artificial tears are similar to your own tears. They lubricate the eyes and help maintain moisture. Artificial tears are available without a prescription. There are many brands on the market, so you may want to try several to find the one you like best.
Preservative-free eyedrops are available for people who are sensitive to the preservatives in artificial tears. If you need to use artificial tears more than every two hours, preservative-free brands may be better for you.
You can use the artificial tears as often as necessary — once or twice a day or as often as several times an hour.
Conserving your tears
Conserving your eyes’ own tears is another approach to keeping the eyes moist. Tears drain out of the eye through a small channel into the nose (which is why your nose runs when you cry). Your ophthalmologist may close these channels either temporarily or permanently with punctal plugs. This method conserves your own tears and makes artificial tears last longer.
Other methods
Tears evaporate like any other liquid. You can take steps to prevent evaporation. In winter, when indoor heating is in use, a humidifier or a pan of water on the radiator adds moisture to dry air. Wraparound glasses may reduce the drying effect of the wind.
A person with dry eye should avoid anything that may cause dryness, such as an overly warm room, hair dryers or wind. Smoking is especially bothersome.
Some people may find dry-eye relief by supplementing their diet found naturally in foods like oily fish (salmon, sardines, anchovies) and flax seeds. Ask your Eye M.D. if you should take supplements of omega-3 fatty acids and, if so, in what form and dosage.
If other methods do not give you adequate relief from dry eye, your ophthalmologist may suggest that you use a prescription medication. One such medication, cyclosporine, works by stimulating tear production. Steroid eyedrops may also be used, but are generally not recommended for long-term treatment. Other treatment options may include ointments, gels and inserts.
Dry eye due to lack of vitamin A in the diet is rare in the United States but is more common in poorer countries, especially among children. Ointments containing vitamin A can help dry eye if it is caused by unusual conditions such as Stevens-Johnson syndrome or pemphigoid. Vitamin A supplements do not seem to help people with ordinary dry eye.
If you are bothered by dry eye, talk with your eye doctor for ways to find relief.
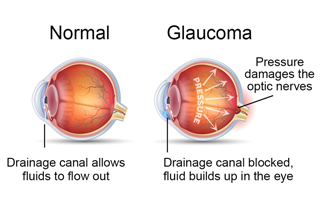
Glaucoma is a disease that damages the eye’s optic nerve. The optic nerve is connected to the retina — a layer of light-sensitive tissue lining the back of the eye. The optic nerve is made up of many nerve fibers, like an electric cable is made up of many wires. The optic nerve sends signals from your retina to your brain, where these signals are interpreted as the images you see.
In the healthy eye, a clear fluid called aqueous (pronounced AY-kwee-us) humor circulates inside the front portion of your eye. To maintain a constant healthy eye pressure, your eye continually produces a small amount of aqueous humor while an equal amount of this fluid flows out of your eye
The fluid flows out through a very tiny drain called the trabecular meshwork, a complex network of cells and tissue in an area called the drainage angle.
If you have glaucoma, the aqueous humor does not flow through the trabecular meshwork properly. Fluid pressure in the eye builds up and over time causes damage to the nerve fibers.
Glaucoma can cause blindness if it is left untreated. Only about half of the three million Americans who have glaucoma are even aware that they have the condition.
When glaucoma develops, usually you don’t have any early symptoms and the disease progresses slowly. In this way, glaucoma can steal your sight very gradually. Fortunately, early detection and treatment can help preserve your vision.
There are several types of glaucoma:
Open-angle glaucoma
The most common form of glaucoma is called primary open-angle glaucoma. It occurs when the trabecular meshwork of the eye gradually becomes less efficient at draining fluid. As this happens, your eye pressure, called intraocular pressure (IOP), rises. Raised eye pressure leads to damage of the optic nerve. Damage to the optic nerve can occur at different eye pressures among different patients. Your ophthalmologist establishes a target eye pressure for you that he or she predicts will protect your optic nerve from further damage. Different patients have different target pressures.
Typically, open-angle glaucoma has no symptoms in its early stages and your vision remains normal. As the optic nerve becomes more damaged, blank spots begin to appear in your field of vision. You usually won’t notice these blank spots in your day-to-day activities until the optic nerve is significantly damaged and these spots become large. If all of the optic nerve fibers die, blindness results.
Half of patients with glaucoma do not have high eye pressure when first examined. That is why it is essential that the optic nerve be examined by an ophthalmologist for proper diagnosis.
Normal-tension glaucoma
Eye pressure is expressed in millimeters of mercury (mm Hg), the same unit of measurement used in weather barometers.
Although normal eye pressure is considered a measurement less than 21 mm Hg, this can be misleading. Some people have a type of glaucoma called normal-tension, or low-tension glaucoma. Their eye pressure is consistently below 21 mm Hg, but optic nerve damage and visual field loss still occur. People with normal-tension glaucoma typically receive the same methods of treatment used for open-angle glaucoma.
Conversely, ocular hypertension is a condition where someone has higher eye pressure than normal, but does not have other signs of glaucoma, such as optic nerve damage or blank spots that show up in their peripheral (side) vision when tested. Someone with ocular hypertension is considered a “glaucoma suspect” because he or she may be at risk for developing glaucoma later. Just like people with glaucoma, people with ocular hypertension need to be closely monitored by an ophthalmologist to ensure they receive appropriate treatment.
Closed-angle glaucoma
A less common form of glaucoma is closed-angle, or narrow-angle, glaucoma. Closed-angle glaucoma occurs when the drainage angle of the eye becomes blocked. Unlike open-angle glaucoma, eye pressure usually goes up very fast. The pressure rises because the iris — the colored part of the eye — partially or completely blocks off the drainage angle. People of Asian descent and those with hyperopia (farsightedness) tend to be more at risk for developing this form of glaucoma.
If the drainage angle becomes completely blocked, eye pressure rises quickly resulting in a closed-angle glaucoma attack. Symptoms of an attack include:
- Severe eye or brow pain;
- Redness of the eye;
- Decreased or blurred vision;
- Seeing colored rainbows or halos;
- Headache;
- Nausea;
- Vomiting.
A closed-angle glaucoma attack is a medical emergency and must be treated immediately. Unfortunately, people at risk for developing closed-angle glaucoma often have few or no symptoms before the attack.
People at risk for closed-angle glaucoma should avoid over-the-counter decongestants and other medications where the packaging states not to use these products if you have glaucoma.
Congenital glaucoma
Congenital glaucoma is a rare type of glaucoma that develops in infants and young children. It happens when the eye’s drainage system doesn’t develop fully or correctly before birth. Congenital glaucoma can be inherited.
Secondary glaucoma
Glaucoma can often develop as the result of another eye condition or disease. This is known as secondary glaucoma. For example, someone who has a tumor or people undergoing long-term steroid therapy may develop secondary glaucoma. Other causes of secondary glaucoma include:
- Eye injury;
- Inflammation of the eye;
- Abnormal blood vessel formation from diabetes or retinal blood vessel blockage;
- Use of steroid-containing medications (pills, eyedrops, sprays);
- Pigment dispersion: tiny fragments or granules from the iris (the colored part of the eye) can circulate in the aqueous humor (the fluid within the front portion of the eye) and block the trabecular meshwork, the tiny drain for the eye’s aqueous humor.
In its early stages, glaucoma has no symptoms. As the disease progresses and more damage occurs, blind spots develop in your peripheral (side) vision. These spots may not be noticeable until the optic nerve has become severely damaged — or until detected by an ophthalmologist during a complete exam.
People at risk for closed-angle glaucoma, where the eye’s drainage angle becomes blocked, usually have no symptoms before the attack, though some early symptoms can include blurred vision, halos, headache or mild eye pain or redness. At the time of a closed-angle glaucoma attack, symptoms include:
- Severe eye or brow pain;
- Redness of the eye;
- Decreased or blurred vision;
- Seeing colored rainbows or halos;
- Headache;
- Nausea;
- Vomiting.
People with “normal-tension glaucoma” may have eye pressures within normal ranges, but have glaucoma signs and symptoms, such as blind spots in their field of vision and optic nerve damage.
Some people may not have glaucoma symptoms, but may have higher than normal eye pressure (called ocular hypertension). They are considered “glaucoma suspects,” and should be monitored carefully by an ophthalmologist.
Some people are at greater risk for developing glaucoma and should see their ophthalmologist on a regular basis, specifically for glaucoma testing. Risk factors for glaucoma include:
- Age;
- Family history of glaucoma;
- African or Hispanic ancestry;
- Farsightedness or nearsightedness;
- Elevated eye pressure;
- Past eye injury;
- Having a thinner central cornea (the clear, front part of the eye covering the pupil and colored iris);
- Not having eye examinations when they are recommended;
- Low blood pressure;
- Conditions that affect blood flow, such as migraines diabetes low blood pressure.
One of the problems with glaucoma, especially open-angle glaucoma, is that there are typically no symptoms in the early stages. Many people who have the disease do not know they have it. This is why it is important, especially as you get older, to have regular medical eye exams by an ophthalmologist.
The eye examination
In a glaucoma evaluation, your doctor:
- Measures the pressure in your eye (tonometry);
- Inspects your eye’s drainage angle (gonioscopy);
- Inspects your optic nerve (ophthalmoscopy);
- Tests your side, or peripheral, vision (visual field test);
- Measures the thickness of your cornea — the clear window at the front of the eye (pachymetry).
Tonometry exam
Your doctor measures your eye pressure using tonometry. Testing your eye pressure is an important part of a glaucoma evaluation. A high pressure reading is often the first sign that you have glaucoma.
During this test, your eye is numbed with eyedrops. Your doctor uses an instrument called a tonometer to measure eye pressure. The instrument measures how your cornea resists pressure.
Normal eye pressure generally ranges between 10 and 21 mm Hg. However, people with normal-tension glaucoma can have damage to their optic nerve and visual field loss even though their eye pressure remains consistently lower than 21 mm Hg.
Gonioscopy exam
Gonioscopy allows your ophthalmologist to get a clear look at the drainage angle to determine the type of glaucoma you may have. Your ophthalmologist is not able to see your eye’s drainage angle by looking at the front of your eye. However, by using a mirrored lens, your ophthalmologist can examine
the drainage angle to determine if you have open-angle glaucoma (where the drainage angle is not working efficiently enough), closed-angle glaucoma (where the drainage angle is at least partially blocked), or a dangerously narrow angle (where the iris is so close to the eye’s drain that the iris could block it).

Ophthalmoscopy exam
Your ophthalmologist inspects your optic nerve for signs of damage using an ophthalmoscope, an instrument that magnifies the interior of the eye. Your pupils will be dilated (widened) with eyedrops to allow your doctor a better view of your optic nerve.
A normal optic nerve is made up of more than one million tiny nerve fibers. As glaucoma damages the optic nerve, it causes the death of some of these nerve fibers. As a result, the appearance of the optic nerve changes. This is referred to as cupping. As the cupping increases, blank spots begin to develop in your field of vision.

Visual field test
The visual field test will check for blank spots in your vision. The results of the test show your ophthalmologist if and where blank spots appear in your field of vision — including spots you may not even notice.
The test is performed using a bowl-shaped instrument called a perimeter. When taking the test, a patch is temporarily placed on one of your eyes so that only one eye is tested at a time. You will be seated and asked to look straight ahead at a target. Random points of light will flash around the bowl-shaped perimeter, and you will be asked to press a button whenever you see a light. Visual field testing is usually performed every 6 to 12 months to monitor for change.
Pachymetry
Because the thickness of the cornea can affect eye pressure readings, pachymetry is used to measure corneal thickness. A probe called a pachymeter is gently placed on the cornea to measure its thickness.
Early detection and treatment can protect your vision.
People of any age with symptoms of or risk factors for glaucoma, such as those with diabetes, a family history of glaucoma, or those of African descent, should see an ophthalmologist for an exam. Your ophthalmologist will let you know how often to return for follow-up exams.
Adults with no symptoms of or risk factors for eye disease should have a complete eye disease screening by age 40
the time when early signs of disease and changes in vision may start to happen. Based on the results of the initial screening, your ophthalmologist will let you know how often to return for follow-up exams.
Adults 65 or older should have an eye exam every one to two years, or as recommended by your ophthalmologist.
If you have glaucoma, preserving your vision requires strong teamwork between you and your doctor. Your doctor can prescribe treatment, but it’s important to do your part by following your treatment plan closely. Be sure to take your medications as prescribed and see your ophthalmologist regularly.

How your glaucoma is treated will depend on your specific type of glaucoma, the severity of your disease, and how it responds to treatment.
Medicine
Medicated eyedrops are the most common way to treat glaucoma. These medications lower your eye pressure in one of two ways — either by slowing the production of aqueous humor or by improving the flow through the drainage angle.
These eyedrops must be taken every day. Just like any other medication, it is important to take your eyedrops regularly as prescribed by your ophthalmologist.
Never change or stop taking your medications without consulting your doctor. If you are about to run out of your medication, ask your doctor if you should have it refilled.
It is important to tell your ophthalmologist about your other medical conditions and all other medications you currently take. Bring a list of your medications with you to your eye appointment. Also tell your primary care doctor and any other doctors caring for you, what glaucoma medication you take.
Surgery
In some patients with glaucoma, surgery is recommended. Glaucoma surgery improves the flow of fluid out of the eye, resulting in lower eye pressure.
Laser trabeculoplasty
To treat open-angle glaucoma, a surgery called laser trabeculoplasty is often used. There are two types of trabeculoplasty surgery: argon laser trabeculoplasty (ALT) and selective laser trabeculoplasty (SLT).
During ALT surgery, a laser makes tiny, evenly spaced burns in the trabecular meshwork. The laser does not create new drainage holes, but rather stimulates the drain to function more efficiently.
With SLT, a laser is used at different frequencies, allowing it to work at very low levels. SLT treats specific cells and leaves the mesh-like drainage canals surrounding the iris intact. SLT may be an alternative for those who have been treated unsuccessfully with traditional laser surgery or with pressure-lowering drops.
Even if laser trabeculoplasty is successful, most patients continue taking glaucoma medications after surgery. For many, this surgery is not a permanent solution. Nearly half who receive this surgery develop increased eye pressure again within five years. Many people who have had a successful laser trabeculoplasty have a repeat treatment. Laser trabeculoplasty can also be used as a first line of treatment for patients who are unwilling or unable to use eyedrops.
An eye that has a peripheral iridectomy. The arrow points to the area where the small piece of iris was removed.
Laser iridotomy
Laser iridotomy is recommended for treating people with closed-angle glaucoma and those with very narrow drainage angles. A laser creates a small hole about the size of a pinhead through the top part of the iris to improve the flow of aqueous fluid to the drainage angle. This hole is hidden from view by the upper eyelid.
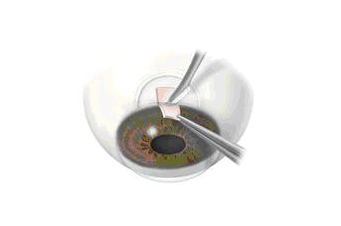
In trabeculectomy, a flap is first created in the sclera (the white part of the eye). Then a small opening is made into the eye to release fluid from the eye.
Peripheral iridectomy
When laser iridotomy is unable to stop an acute closed-angle glaucoma attack, or is not possible for other reasons, a peripheral iridectomy may be performed. Performed in an operating room, a small piece of the iris is removed, giving the aqueous fluid access to the drainage angle again. Because most cases of closed-angle glaucoma can be treated with medications and laser iridotomy, peripheral iridectomy is rarely necessary.
Trabeculectomy
In trabeculectomy, a small flap is made in the sclera (the outer white coating of your eye). A filtration bleb, or reservoir, is created under the conjunctiva — the thin, filmy membrane that covers the white part of your eye. Once created, the bleb looks like a bump or blister on the white part of the eye above the iris, but the upper eyelid usually covers it. The aqueous humor can now drain through the flap made in the sclera and collect in the bleb, where the fluid will be absorbed into blood vessels around the eye.
During surgery, the scleral flap is closed with tiny stitches. Some of these stitches may be removed after surgery to increase drainage. Medication to reduce scarring is often used during and after surgery.
Eye pressure is effectively controlled in three out of four people who have trabeculectomy. Although regular follow-up visits with your doctor are still necessary, many patients no longer need to use eyedrops. If the new drainage channel closes or too much fluid begins to drain from the eye, additional surgery may be needed.
Aqueous shunt surgery
If trabeculectomy cannot be performed, aqueous shunt surgery is usually successful in lowering eye pressure. An aqueous shunt is a small plastic tube or valve connected on one end to a reservoir (a roundish or oval plate). The shunt is an artificial drainage device and is implanted in the eye through a tiny incision. The shunt redirects aqueous humor to an area beneath the conjunctiva (the thin membrane that covers the inside of your eyelids and the white part of your eye). The fluid is then absorbed into the blood vessels. When healed, the reservoir is not easily seen unless you look downward and lift your eyelid.
Important things to remember about glaucoma:
- Vision loss from glaucoma usually can be prevented if it is detected and treated early enough.
- If you use eyedrops to treat glaucoma, be sure to continue taking the medication as your doctor tells you to. Never change or stop taking your medications without consulting your doctor.
- There are a number of ways to treat glaucoma. While some people may experience side effects from medications or surgery, the risks of side effects should always be balanced with the greater risk of leaving glaucoma untreated and losing vision.


